European Commission Approves IMBRUVICATM in Two Forms of Blood Cancer
First-in-class BTK inhibitor for complex orphan diseases CLL and MCL
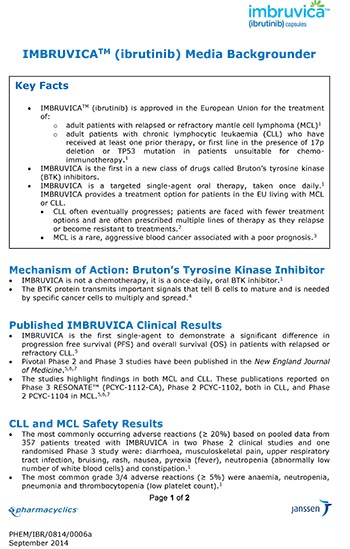
BEERSE, Belgium, October 17, 2014 /PRNewswire/ – Janssen-Cilag International NV (Janssen) announced today that the European Commission has approved IMBRUVICA™ (ibrutinib) capsules, a first-in-class, once-daily, oral Bruton’s tyrosine kinase (BTK) inhibitor. This new approach to treating blood cancers works by blocking BTK, a protein that helps certain cancer cells live and grow.1 IMBRUVICA is indicated for the treatment of adult patients with relapsed or refractory mantle cell lymphoma (MCL), or adult patients with chronic lymphocytic leukaemia (CLL) who have received at least one prior therapy, or in first line in the presence of 17p deletion or TP53 mutation in patients unsuitable for chemo-immunotherapy.2
IMBRUVICA is co-developed by Cilag GmbH International (a member of the Janssen Pharmaceutical Companies) and Pharmacyclics Switzerland GmbH. In the European Economic Area, Janssen is the marketing authorisation holder. Janssen affiliates market IMBRUVICA in EMEA (Europe, Middle East and Africa) as well as the rest of the world, except for the United States, where both companies co-market it.
The decision from the European Commission follows a positive opinion from the Committee for Medicinal Products for Human Use (CHMP) of the European Medicines Agency (EMA) on 24 July 2014.2 This approval allows for the marketing of IMBRUVICA in all 28 countries of the European Union.
“MCL and CLL with 17p deletion are usually challenging and difficult-to-treat blood cancers that do not respond well to conventional therapies. They usually rapidly progress during or soon after chemotherapy leaving patients with very limited treatment options and poor survival,” said Professor Peter Hillmen, Haematology, St. James’s University Hospital, Leeds, who is an investigator in the IMBRUVICA CLL clinical trial. "Being able to use IMBRUVICA as a single agent offers a new option and gives renewed hope for physicians and their patients.”
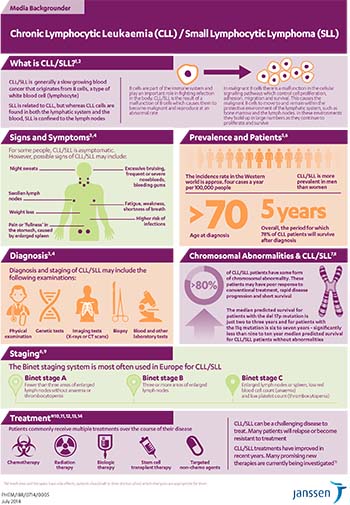
CLL in most patients is a slow-growing blood cancer, starting from white blood cells (called lymphocytes) in the bone marrow.3 The chromosomal abnormalities deletion 17p (del17p) and TP53 mutation are associated with aggressive, treatment-resistant disease.4 MCL is a rare and aggressive type of B-cell lymphoma that can be challenging to treat and is associated with a poor prognosis.5,6
The approval of IMBRUVICA was based on data from the Phase 3 (RESONATE™ PCYC-1112) and Phase 1b-2 (PCYC-1102) studies in CLL, and the Phase 2 study (PCYC-1104) in MCL.
“We are delighted the European Commission has approved IMBRUVICA as a new treatment approach, which could prolong the lives of patients with these complex blood cancers,” said Jane Griffiths, Company Group Chairman, Janssen, Europe, Middle East and Africa (EMEA). "This is a positive step forward for patients, and Janssen is committed to looking into further areas of unmet need in blood cancers where IMBRUVICA could improve outcomes.”
NOTES TO EDITORS
CLL Study and Efficacy Results
RESONATE™ (PCYC-1112) is a Phase 3, multi-centre, international, open-label, randomised study that examined ibrutinib as a single agent (given orally) versus ofatumumab (given intravenously) in relapsed or refractory patients with CLL (n=391).7
The results from the study showed that at a median follow up of 9.4 months, single agent ibrutinib significantly improved progression-free survival (PFS), overall survival (OS) and overall response rate (ORR) in this difficult-to-treat patient population, regardless of baseline characteristics [ORR was assessed according to the 2008 International Workshop on CLL (IWCLL) criteria by investigators and an independent review committee (IRC)].7,8
The median PFS in the ofatumumab arm was 8.1 months and was not reached in the ibrutinib arm because progression events occurred more slowly. The PFS results represent a 78 percent reduction in the risk of progression or death in patients treated with ibrutinib compared to ofatumumab.7 The OS median was not reached in either arm, but at a median follow up of 9.4 months the results showed a 57 percent reduction in the risk of death in patients receiving ibrutinib versus those receiving ofatumumab. Results were consistent across all baseline sub-groups, including those with del17p.7
MCL Study and Efficacy Results
The efficacy of ibrutinib in patients with relapsed or refractory MCL was evaluated in an open-label, multi-centre, single-arm Phase 2 study (PCYC-1104) of 111 treated patients. An overall response rate of 68 percent was observed, with a complete response rate of 21 percent and a partial response rate of 47 percent. With a median follow up of 15.3 months, the median duration of response was 17.5 months; the median progression-free survival was 13.9 months.9
CLL and MCL Safety Results
The most commonly occurring adverse reactions (≥ 20 percent) were diarrhoea, musculoskeletal pain, upper respiratory tract infection, bruising, rash, nausea, pyrexia (fever), neutropenia (abnormally low number of white blood cells) and constipation. The most common grade 3/4 adverse reactions (≥ 5 percent) were anaemia, neutropenia, pneumonia and thrombocytopenia (low platelet count).7,9
About IMBRUVICA™
IMBRUVICA (ibrutinib) is a Bruton's tyrosine kinase (BTK) inhibitor, which works by forming a strong covalent bond with BTK to block the transmission of cell survival signals within the malignant B cells.1 By blocking this BTK protein, IMBRUVICA helps kill and reduce the number of cancer cells. It also slows down the worsening of the cancer.10
Investigational uses for ibrutinib, alone and in combination with other treatments, are underway in several blood cancers including CLL, MCL, Waldenström's macroglobulinemia (WM), diffuse large B-cell lymphoma (DLBCL), follicular lymphoma (FL) and multiple myeloma (MM); IMBRUVICA is approved for the treatment of CLL and MCL; regulatory approval for additional uses has not yet been granted.
IMBRUVICA received U.S. Food and Drug Administration (FDA) approval for the treatment of patients with MCL in November 2013 and conditional approval for the treatment of CLL in patients who have received at least one prior therapy in February 2014. Regular approval in CLL followed in July 2014, including approval as a first-line therapy in del17p patients. IMBRUVICA is also approved in Israel for the treatment of adult patients with MCL or CLL who have received at least one prior treatment.
About CLL
In most patients, CLL is generally a slow-growing blood cancer of the white blood cells called B-lymphocytes. The median age at diagnosis is 72 years, and incidence rates among men and women in Europe are approximately 5.87 and 4.01 cases per 100,000 persons per year, respectively.3,11,12 CLL is a chronic disease; median overall survival ranges between 18 months and more than 10 years according to the stage of disease.13 The disease eventually progresses in the majority of patients, and patients are faced with fewer treatment options each time. Patients are often prescribed multiple lines of therapy as they relapse or become resistant to treatments.
Deletion 17p (del17p) and TP53 mutation are associated with aggressive, treatment-resistant disease. The abnormality results in the loss of function of a key gene, TP53. TP53 senses the presence of abnormal DNA and triggers either DNA repair mechanisms or cell death and is important in tumour suppression and the action of cytotoxic chemotherapy.4 Approximately five to eight percent of patients receiving first-line treatment have del17p at diagnosis. However, incidence of del17p and/or TP53 mutation rises to 29 to 52 percent in patients who have relapsed or refractory disease.14 The median predicted survival for patients with the del17p mutation or TP53 mutation is just two to three years.11
CLL cells are found in both the lymphatic system and the blood.15 When the cancer cells are located mostly in the lymph nodes, the disease is called small lymphocytic lymphoma (SLL). Both CLL and SLL are considered different manifestations of the same entity, as classified in the fourth edition of the World Health Organization Classification of Tumours of Haematopoietic and Lymphoid Tissues.16
About MCL
MCL is considered a rare disease, characterised by high unmet need and small patient populations impacting fewer than one in 200,000 people in Europe and with a median age at diagnosis of 65.17,18 MCL is much more predominant in men than women and accounts for three to 10 percent of all non-Hodgkin’s lymphomas.19,20 Median overall survival is typically three to four years, and only one to two years in patients following the first relapse.18 MCL typically involves the lymph nodes, but can spread to other tissues, such as the bone marrow, liver, spleen and gastrointestinal tract.21 This challenging disease is associated with poor prognoses.
Janssen in Oncology
In oncology, our goal is to fundamentally alter the way cancer is understood, diagnosed, and managed, reinforcing our commitment to the patients who inspire us. In looking to find innovative ways to address the cancer challenge, our primary efforts focus on several treatment and prevention solutions. These include a focus on haematologic malignancies, prostate cancer and lung cancer; cancer interception with the goal of developing products that interrupt the carcinogenic process; biomarkers that may help guide targeted, individualised use of our therapies; as well as safe and effective identification and treatment of early changes in the tumour microenvironment.
About Janssen
Janssen Pharmaceutical Companies of Johnson & Johnson are dedicated to addressing and solving the most important unmet medical needs of our time, including oncology (e.g., multiple myeloma and prostate cancer), immunology (e.g., psoriasis), neuroscience (e.g., schizophrenia, dementia and pain), infectious disease (e.g., HIV/AIDS, hepatitis C and tuberculosis), and cardiovascular and metabolic diseases (e.g., diabetes). Driven by our commitment to patients, we develop sustainable, integrated healthcare solutions by working side-by-side with healthcare stakeholders, based on partnerships of trust and transparency. More information can be found on www.janssen-emea.com. Follow us on www.twitter.com/janssenEMEA for our latest news.
(This press release contains "forward-looking statements" as defined in the Private Securities Litigation Reform Act of 1995 regarding product development. The reader is cautioned not to rely on these forward-looking statements. These statements are based on current expectations of future events. If underlying assumptions prove inaccurate or known or unknown risks or uncertainties materialize, actual results could vary materially from the expectations and projections of Janssen-Cilag International NV, any of the other Janssen Pharmaceutical Companies, and/or Johnson & Johnson. Risks and uncertainties include, but are not limited to: challenges inherent in new product development, including obtaining regulatory approvals; competition, including technological advances, new products and patents attained by competitors; challenges to patents; changes in behavior and spending patterns or financial distress of purchasers of health care products and services; changes to regulations and domestic and foreign health care reforms; and general industry conditions, including trends toward health care cost containment. A further list and description of these risks, uncertainties and other factors can be found in Johnson & Johnson’s Annual Report on Form 10-K for the fiscal year ended December 29, 2013, including in Exhibit 99 thereto, and the company’s subsequent filings with the Securities and Exchange Commission. Copies of these filings are available online at www.sec.gov, www.jnj.com or on request from Johnson & Johnson. None of the Janssen Pharmaceutical Companies or Johnson & Johnson undertakes to update any forward-looking statement as a result of new information or future events or developments.)
REFERENCES
- Akinleye A, Chen Y, Mukhi N, Song Y, Liu D. Ibrutinib and novel BTK inhibitors in clinical development. J Hematol Oncol 2013;6:59.
- European Medicines Agency. Committee for Medicinal Products for Human Use: Summary of opinion. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/Summary_of_opinion_-_Initial_authorisation/human/003791/WC500170191.pdf. Accessed October 2014.
- American Cancer Society. What is chronic lymphocytic leukemia? Available at: http://www.cancer.org/cancer/leukemia-chroniclymphocyticcll/detailedguide/leukemia-chronic-lymphocytic-what-is-cll. Last accessed July 2014.
- Schnaiter A, Stilgenbauer S. 17p Deletion in chronic lymphocytic leukemia: risk stratification and therapeutic approach. Hematol Oncol Clin N Am 2013;27:289-301.
- McKay P, Leach M, Jackson R, et al. Guidelines for the investigation and management of mantle cell lymphoma. Br J Haematol. 2012;159:405-26.
- Williams ME, Dreyling M, Winter J, Muneer S, Leonard JP. Management of mantle cell lymphoma: key challenges and next steps. Clin Lymphoma Myeloma Leuk. 2010;10:336-46.
- Byrd JC, Brown JR, O’Brien S, et al. Ibrutinib versus ofatumumab in previously treated chronic lymphoid leukemia. N Engl J Med. 2014 May 31 [epub ahead of print].
- IMBRUVICA™ (ibrutinib) Summary of Product Characteristics. October 2014.
- Wang ML, Rule S, Martin P, et al. Targeting BTK with ibrutinib in relapsed or refractory mantle-cell lymphoma. N Engl J Med 2013;369:507-16.
- European Medicines Agency. How is the medicine expected to work? http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/orphans/2012/06/human_orphan_001058.jsp&mid=WC0b01ac058001d12b. Accessed September 2014
- Eichhorst B, Dreyling M, Robak T, Montserrat E, Hallek M; ESMO Guidelines Working Group. Chronic lymphocytic leukemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2011;22(Suppl.6):vi50-4.
- Sant M, Allemani C, Tereanu C, et al. Incidence of hematologic malignancies in Europe by morphologic subtype: results of the HAEMACARE project. Blood 2010;116:3724-34.
- Sagatys EM, Zhang L. Clinical and laboratory prognostic indicators in chronic lymphocytic leukemia. Cancer Control 2012;19:18-25.Stilgenbauer S, Zenz T. Understanding and Managing Ultra High-Risk Chronic Lymphocytic Leukemia. Hematology 2010;481-8.
- Stilgenbauer S, Zenz T. Understanding and Managing Ultra High-Risk Chronic Lymphocytic Leukemia. Hematology 2010;481-8.
- Hallek M. Signaling the end of chronic lymphocytic leukemia: new frontline. Blood. 2013;112(23).
- Santos FPS, O’Brien S. Small Lymphocytic Lymphoma and Chronic Lymphocytic Leukemia Are They the Same Disease? The Cancer Journal. 2012;8(5):396-403.
- Smedby KE, Hjalgrim H. Epidemiology and etiology of mantle cell lymphoma and other non-Hodgkin lymphoma subtypes. Semin Cancer Biol 2011;21:293-8.
- Leukemia and Lymphoma Society. Mantle cell lymphoma facts. Available at: http://www.lls.org/content/nationalcontent/resourcecenter/freeeducationmaterials/lymphoma/pdf/mantlecelllymphoma.pdf Last accessed May 14, 2013.
- Swerdlow SH, Campo E, Muller-Hermelink HK. Mantle cell lymphoma. In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri S, Stein M, Thiele J, Vardiman JW, editors. WHO classification of tumors of haematopoietic and lymphoid tissues. Lyon, France: IARC Press; 2008:229–32.
- Vose, J.M. (2012). Mantle cell lymphoma: 2012 update on diagnosis, risk-stratification, and clinical management. Am J Hematol. 87(6): 604-9.
- Goy A, Bernstein SH, Kahl BS, et al. Bortezomib in patients with relapsed or refractory mantle cell lymphoma: updated time-to-event analyses of the multicenter phase 2 PINNACLE study. Ann Oncol 2009;20:520–5.
PHEM/IBR/0814/0006
October 2014
Video Gallery




Mantle Cell Lymphoma (MCL)

Chronic Lymphocytic Leukaemia (CLL)
IMBRUVICA Backgrounder
Translations
FrenchGerman
Spanish
Media Inquiries
Satu Kaarina Glawe
Mobile: +49 (172) 294 6264
Email: [email protected]
Investor Relations:
Stan Panasewicz
Phone: +1 732-524-2524
Louise Mehrotra
Phone: +1 732-524-6491