
Novartis receives FDA approval for Fabhalta® (iptacopan), offering superior hemoglobin improvement in the absence of transfusions as the first oral monotherapy for adults with PNH
- Approval based on APPLY-PNH trial in adults with PNH and anemia despite prior anti-C5 treatment, and supported by the APPOINT-PNH study in complement inhibitor-naïve patients1-5
- In APPLY-PNH, patients who switched to Fabhalta experienced superior increases of hemoglobin levels ≥ 2 g/dL (82.3% vs. 0%) and hemoglobin level ≥ 12 g/dL (67.7% vs. 0%), both in the absence of red blood cell transfusions, vs. patients who continued on anti-C5 treatment1,2
- Fabhalta, now available for both previously treated and treatment-naïve patients, is the only FDA-approved Factor B inhibitor of the immune system’s complement pathway, which drives complement-mediated hemolysis in PNH1,6
- Significant unmet need remains in PNH, a chronic and rare blood disorder; despite anti-C5 therapy, a large proportion of patients can remain anemic and dependent on blood transfusions7,8
- Late-stage Fabhalta development program ongoing in multiple complement-mediated conditions
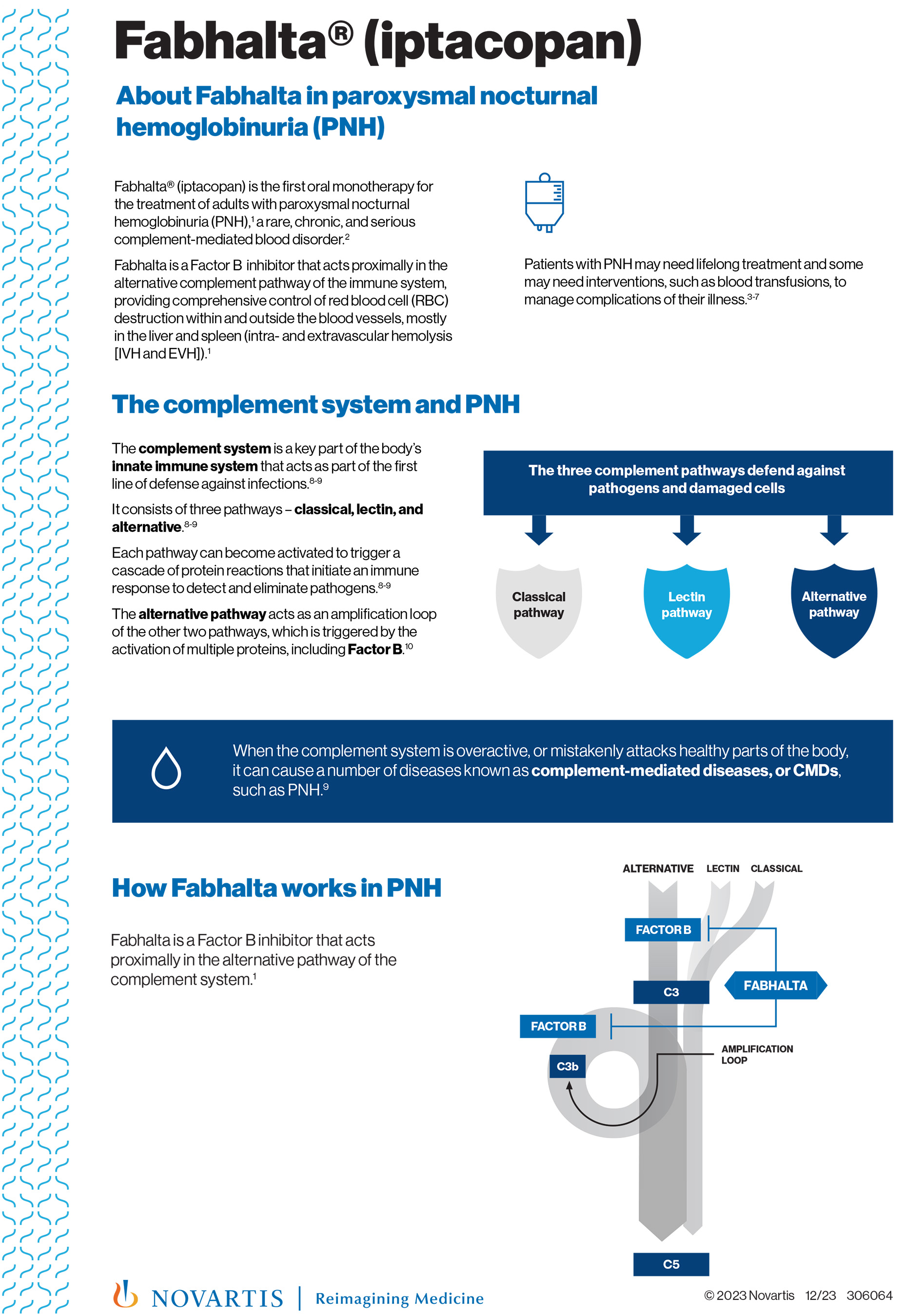
East Hanover, N.J., December 05, 2023 — Novartis today announced that the U.S. Food and Drug Administration (FDA) approved Fabhalta® (iptacopan) as the first oral monotherapy for the treatment of adults with paroxysmal nocturnal hemoglobinuria (PNH)1. Fabhalta is a Factor B inhibitor that acts proximally in the alternative complement pathway of the immune system, providing comprehensive control of red blood cell (RBC) destruction within and outside the blood vessels (intra- and extravascular hemolysis [IVH and EVH]). In clinical trials, treatment with Fabhalta increased hemoglobin levels (≥ 2 g/dL from baseline in the absence of RBC transfusions) in the majority of patients and in APPLY-PNH nearly all patients treated with Fabhalta did not receive blood transfusions1-5.
“An efficacious oral treatment with a demonstrated safety profile could be practice-changing for physicians and help relieve burdens experienced by people with PNH,” said Vinod Pullarkat, MD, MRCP, Clinical Professor, Department of Hematology and Hematopoietic Cell Transplantation, City of Hope. “In clinical studies, iptacopan was superior to anti-C5s in hemoglobin improvement in the absence of RBC transfusion and transfusion avoidance rate, and also effective in complement inhibitor-naïve individuals, by providing clinically meaningful hemoglobin-level increases without the need for blood transfusions.”
The FDA approval is based on the Phase III APPLY-PNH trial in patients with residual anemia (hemoglobin < 10 g/dL) despite prior anti-C5 treatment who switched to Fabhalta, which demonstrated superiority in hemoglobin improvement in the absence of RBC transfusions and in transfusion avoidance rate over patients who stayed on anti-C5 treatments1,2. Approval was also supported by the Phase III APPOINT-PNH study in complement inhibitor-naïve patients1,3. The 24-week core treatment periods in APPLY-PNH and APPOINT-PNH trials respectively showed1-3:
- Patients with sustained increase of hemoglobin levels ≥ 2 g/dLa from baseline in the absence of transfusions: 82.3% of anti-C5-experienced Fabhalta patients responded vs. 0% for anti-C5 (difference of 81.5%b, P<0.0001); 77.5% of complement inhibitor-naïve patients using Fabhalta achieved this outcome (sensitivity analysis showed 87.5%c)1-3.
- Patients with sustained hemoglobin level ≥ 12 g/dLa in the absence of transfusions: 67.7% of anti-C5-experienced Fabhalta patients responded vs. 0% for anti-C5 (difference of 66.6%b, P<0.0001)1-2.
- Patients avoiding transfusiond,e: Transfusion avoidance rate 95.2% for anti-C5-experienced Fabhalta patients vs. 45.7% for anti-C5 (difference of 49.5%b, P<0.0001)1-2.
In the APPLY-PNH trial, the most commonly reported (≥10%) adverse reactions (ARs) with Fabhalta vs. anti-C5s were: headachef (19% vs. 3%), nasopharyngitisg (16% vs. 17%), diarrhea (15% vs. 6%), abdominal painf (15% vs. 3%), bacterial infectionh (11% vs. 11%), nausea (10% vs. 3%), and viral infectioni (10% vs. 31%)1,2. In the APPOINT-PNH trial, the most commonly reported ARs (≥10%) were headachef (28%), viral infectioni (18%), nasopharyngitisg (15%), and rashj (10%)1,3. In APPLY-PNH, serious ARs were reported in two (3%) patients with PNH receiving Fabhalta, which included pyelonephritis, urinary tract infection and COVID-191,2. In APPOINT-PNH, serious ARs were reported in two (5%) patients with PNH receiving Fabhalta, which included COVID-19 and bacterial pneumonia1,3. Fabhalta may cause serious infections caused by encapsulated bacteria and is available only through a Risk Evaluation and Mitigation Strategy (REMS) that requires vaccinations for encapsulated bacteria1.
People with PNH have an acquired mutation making red blood cells susceptible to premature destruction by the complement system6,8. PNH is characterized by hemolysis, bone marrow failure, and thrombosis in varying combinations and levels of severity6-8. Existing C5 inhibitor treatments, administered as infusions, may leave PNH symptoms uncontrolled7,8. Up to 88% of patients on anti-C5 treatment may have persistent anemia with over one-third of those patients requiring blood transfusions at least once per year7,8.
“The U.S. approval of Fabhalta is an extraordinary moment for people living with PNH, their loved ones and the healthcare providers who care for them,” said Victor Bultó, President US, Novartis. “This new, effective oral medicine may mean that patients can reset their expectations of living with PNH, a chronic and life-altering blood disease. As Novartis continues to focus on conditions with unmet patient need, we are exploring the potential of Fabhalta in other complement-mediated diseases – with an ultimate goal to drive meaningful change for patients.”
Discovered and developed by Novartis, Fabhalta is expected to be available in the United States in December. Additional regulatory filings and reviews for Fabhalta in PNH are currently underway around the world.
aAssessed between Day 126 and Day 168. bAdjusted difference in proportion. cSensitivity analysis incorporates data from local labs when central labs were not available. dAssessed between Day 14 and Day 168. eTransfusion avoidance is defined as absence of administration of packed-red blood cell transfusions between Day 14 and Day 168. fIncludes similar terms. gNasopharyngitis contains: rhinitis allergic, upper respiratory tract infection, pharyngitis, rhinitis. hBacterial infection contains: pyelonephritis, urinary tract infection, bronchitis bacterial, bronchitis haemophilus, cholecystitis, folliculitis, cellulitis, arthritis bacterial, sepsis, klebsiella infection, staphylococcal infection, Pseudomonas infection, hordeolum, pneumonia bacterial. iViral infection contains: COVID-19, herpes zoster, oral herpes, nasal herpes, influenza A virus test positive, influenza. jRash: dermatitis allergic, acne, erythema multiforme, rash maculo-papular, rash erythematous.
Indication
FABHALTA is a prescription medicine used to treat adults with paroxysmal nocturnal hemoglobinuria (PNH).
It is not known if FABHALTA is safe and effective in children.
Important Safety Information
FABHALTA is a medicine that affects part of the immune system and may lower one’s ability to fight infections. FABHALTA increases the chance of getting serious infections caused by encapsulated bacteria, including Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae type B. These serious infections may quickly become life-threatening or fatal if not recognized and treated early. Patients must complete or update vaccinations against these bacteria at least 2 weeks before starting FABHALTA. If patients have not completed these vaccinations and FABHALTA therapy must be started right away, they should receive the required vaccinations as soon as possible. If patients have not been vaccinated and FABHALTA must be started right away, they should also receive antibiotics to take for as long as their doctor tells them. If patients have been vaccinated against these bacteria in the past, they might need additional vaccinations before starting FABHALTA. Their doctor will decide if they need additional vaccinations. Vaccines do not prevent all infections caused by encapsulated bacteria. Patients should call their doctor or get emergency medical care right away if they have any of these signs and symptoms of a serious infection: fever with or without shivers or chills; fever with chest pain and cough; fever with high heart rate; headache and fever; confusion; clammy skin; fever and a rash; fever with breathlessness/fast breathing; headache with nausea or vomiting; headache with stiff neck or stiff back; body aches with flu-like symptoms; or eyes sensitive to light. Doctors will give their patients a Patient Safety Card about the risk of serious infections. Patients must carry it with them at all times during treatment and for 2 weeks after their last dose of FABHALTA. The risk of serious infections may continue for a few weeks after their last dose of FABHALTA. It is important for patients to show this card to any doctor who treats them. This will help doctors diagnose and treat patients quickly.
FABHALTA is only available through a program called the FABHALTA Risk Evaluation and Mitigation Strategy (REMS). Before patients can take FABHALTA, their doctor must enroll in the FABHALTA REMS program, counsel patients about the risk of serious infections caused by certain bacteria, give patients information about the symptoms of serious infections, make sure that patients are vaccinated against serious infections caused by encapsulated bacteria and that they receive antibiotics if they need to start FABHALTA right away and are not up to date on vaccinations, as well as give patients a Patient Safety Card about the risk of serious infections.
Since FABHALTA may increase patients’ cholesterol and triglycerides, their doctor will do blood tests to check their levels periodically.
Patients should not take FABHALTA if they are allergic to FABHALTA or any of the ingredients in FABHALTA. Patients should not take FABHALTA if they have a serious infection caused by encapsulated bacteria, including Streptococcus pneumoniae, Neisseria meningitidis, or Haemophilus influenzae type B when starting FABHALTA.
Before taking FABHALTA, patients should tell their doctor about all their medical conditions, including if they have an infection or fever, have kidney or liver problems, are pregnant or plan to become pregnant (it is not known if FABHALTA will harm an unborn baby), or are breastfeeding or plan to breastfeed as it is not known if FABHALTA passes into breast milk. Patients should not breastfeed during treatment and for 5 days after the last dose of FABHALTA.
Patients should tell their doctor about all the medicines they take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. Taking FABHALTA with certain other medicines may affect the way FABHALTA works and may cause side effects. Patients should know the medicines they take and the vaccines they receive. Patients should keep a list of them to show their doctor and pharmacist when they get a new medicine.
If patients have PNH and stop taking FABHALTA, their doctor will need to monitor them closely for at least 2 weeks after stopping FABHALTA. Stopping treatment with FABHALTA may cause a breakdown of red blood cells due to PNH. Symptoms or problems that can happen due to breakdown of red blood cells include decreased hemoglobin level in the blood; blood in the urine; shortness of breath; trouble swallowing; tiredness; pain in the stomach (abdomen); blood clots, stroke, and heart attack; and erectile dysfunction (ED). It is important that patients take FABHALTA exactly as their doctor tells them to lower the possibility of breakdown of red blood cells due to PNH.
The most common side effects of FABHALTA include headache; nasal congestion, runny nose, cough, sneezing, and sore throat (nasopharyngitis); diarrhea; pain in the stomach (abdomen); infections (viral and bacterial); nausea; and rash.
Please see full Prescribing Information, including Boxed WARNING and Medication Guide.About APPLY-PNH
APPLY-PNH (NCT04558918) was a Phase III, randomized, multinational, multicenter, active-comparator controlled, open-label trial to evaluate the efficacy and safety of twice-daily, oral Fabhalta monotherapy (200 mg) for the treatment of PNH by assessing if switching to Fabhalta was superior to continuing on anti-C5 therapies (US-approved and non-US-approved eculizumab and ravulizumab) in adult patients presenting with residual anemia (Hb <10 g/dL) despite a stable regimen of anti-C5 treatment in the last six months prior to randomization2,10. The trial enrolled 97 patients who were randomized in an 8:5 ratio to either twice-daily, oral Fabhalta monotherapy, or intravenous anti-C5 therapies (continuing with the same regimen as they were on prior to randomization)2,9.
About APPOINT-PNH
APPOINT-PNH (NCT04820530) was a Phase III, multinational, multicenter, open-label, uncontrolled single-arm study to evaluate the efficacy and safety of twice-daily, oral Fabhalta monotherapy (200 mg) in adult PNH patients who are naïve to complement inhibitor therapy, including anti-C5 therapies (eculizumab or ravulizumab)3,10.The trial enrolled 40 patients who received twice-daily, oral Fabhalta monotherapy3,10.
About paroxysmal nocturnal hemoglobinuria (PNH)
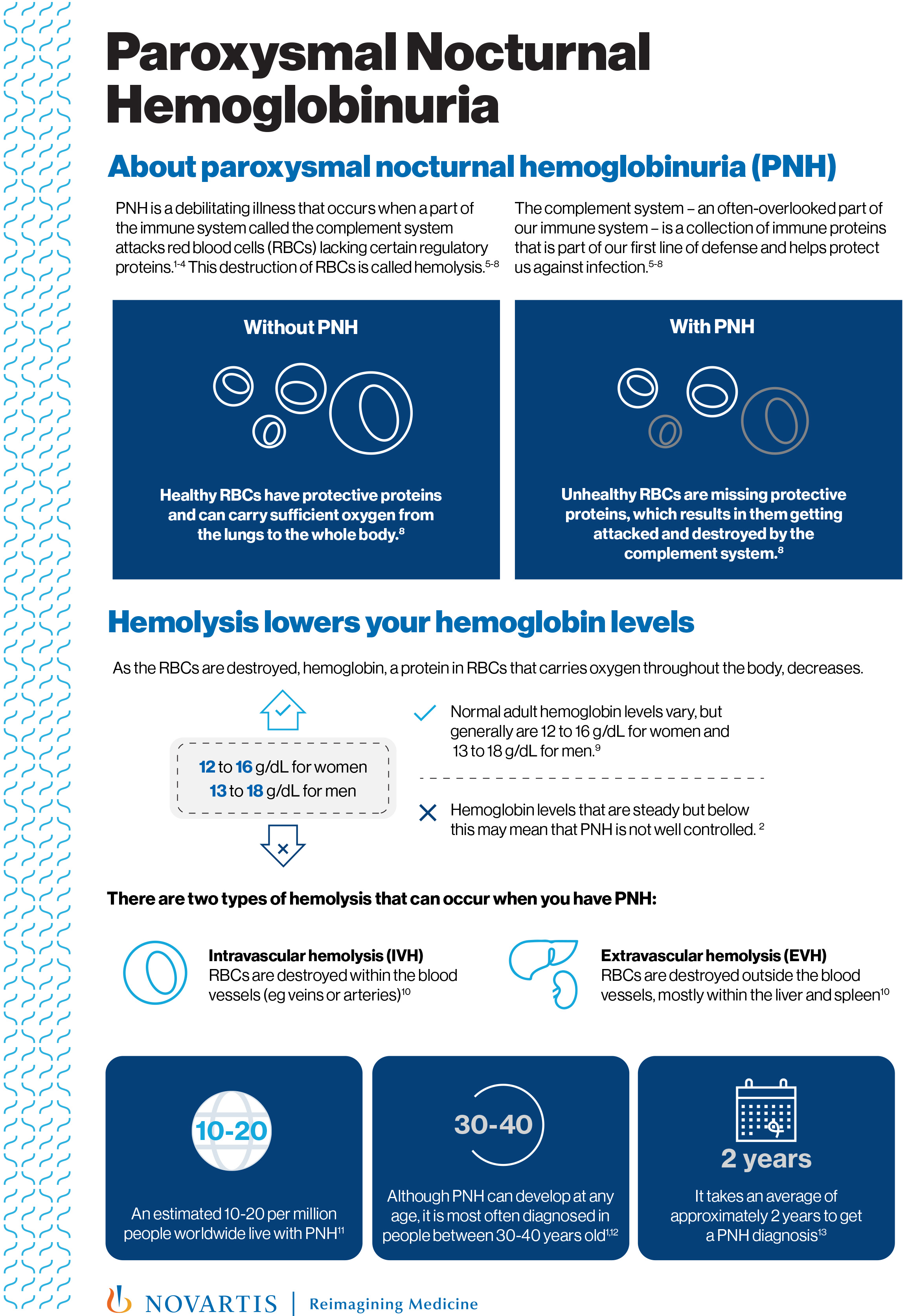
PNH is a rare, chronic and serious complement-mediated blood disorder6. People with PNH have an acquired mutation in some of their hematopoietic stem cells (which are located in the bone marrow and can grow and develop into RBCs, white blood cells and platelets) that causes them to produce RBCs that are susceptible to premature destruction by the complement system6,8. This leads to intravascular hemolysis (destruction of RBCs within blood vessels) and extravascular hemolysis (destruction of RBCs mostly in the spleen and liver), which cause anemia (low levels of circulating RBCs), thrombosis (formation of blood clots) and other debilitating symptoms6,8.
It is estimated that approximately 10-20 people per million worldwide live with PNH6. Although PNH can develop at any age, it is often diagnosed in people between 30-40 years old11,12.
PNH has a significant unmet need not fully addressed by anti-C5 therapies (eculizumab or ravulizumab): despite treatment with anti-C5s, a large proportion of people with PNH may remain anemic, and dependent on blood transfusions6-8,13,14.
About Fabhalta® (iptacopan)
Fabhalta (iptacopan) is an oral, Factor B inhibitor of the alternative complement pathway15-17. Fabhalta is indicated for the treatment of adults with paroxysmal nocturnal hemoglobinuria (PNH).
Discovered at Novartis, Fabhalta is currently in development for a range of complement-mediated diseases including immunoglobulin A nephropathy (IgA nephropathy), C3 glomerulopathy (C3G), immune complex membranoproliferative glomerulonephritis (IC-MPGN) and atypical hemolytic uremic syndrome (aHUS).
Based on disease prevalence, unmet needs and data from Phase II studies, Fabhalta has received FDA Breakthrough Therapy Designation in PNH, FDA Breakthrough Therapy Designation in C3G, orphan drug designations from the FDA and EMA in PNH and C3G, EMA PRIME designation for C3G, and EMA orphan drug designation in IgAN18-21.
Disclaimer
This press release contains forward-looking statements within the meaning of the United States Private Securities Litigation Reform Act of 1995. Forward-looking statements can generally be identified by words such as “potential,” “can,” “will,” “plan,” “may,” “could,” “expectations,” “investigational,” “drives,” “remains,” “ongoing,” “exploring,” “goal,” “expected,” “estimated,” or similar terms, or by express or implied discussions regarding potential marketing approvals, new indications or labeling for FABHALTA (iptacopan), or regarding potential future revenues from FABHALTA (iptacopan). You should not place undue reliance on these statements. Such forward-looking statements are based on our current beliefs and expectations regarding future events, and are subject to significant known and unknown risks and uncertainties. Should one or more of these risks or uncertainties materialize, or should underlying assumptions prove incorrect, actual results may vary materially from those set forth in the forward-looking statements. There can be no guarantee that FABHALTA (iptacopan) will be submitted or approved for sale or for any additional indications or labeling in any market, or at any particular time. Nor can there be any guarantee that FABHALTA (iptacopan)will be commercially successful in the future. In particular, our expectations regarding FABHALTA (iptacopan) could be affected by, among other things, the uncertainties inherent in research and development, including clinical trial results and additional analysis of existing clinical data; regulatory actions or delays or government regulation generally; global trends toward health care cost containment, including government, payor and general public pricing and reimbursement pressures and requirements for increased pricing transparency; our ability to obtain or maintain proprietary intellectual property protection; the particular prescribing preferences of physicians and patients; general political, economic and business conditions, including the effects of and efforts to mitigate pandemic diseases; safety, quality, data integrity or manufacturing issues; potential or actual data security and data privacy breaches, or disruptions of our information technology systems, and other risks and factors referred to in Novartis AG’s current Form 20-F on file with the US Securities and Exchange Commission. Novartis is providing the information in this press release as of this date and does not undertake any obligation to update any forward-looking statements contained in this press release as a result of new information, future events or otherwise.
About Novartis
Novartis is an innovative medicines company. Every day, we work to reimagine medicine to improve and extend people’s lives so that patients, healthcare professionals and societies are empowered in the face of serious disease. Our medicines reach more than 250 million people worldwide.
Reimagine medicine with us: Visit us at https://www.novartis.com and https://www.novartis.us and connect with us on LinkedIn, LinkedIn US, Facebook, X/Twitter, X/Twitter US and Instagram.
References
- Iptacopan Prescribing Information. East Hanover, NJ: Novartis Pharmaceuticals Corp; December 2023.
- Risitano AM, Rӧth A, Kulasekararaj A, et al. Oral Iptacopan Monotherapy Has Superior Efficacy to Anti-C5 Therapy in Patients with Paroxysmal Nocturnal Hemoglobinuria and Residual Anemia: Results From the Phase III APPLY-PNH Study. Presented at: 49th Annual Meeting of the European Society for Blood and Marrow Transplantation (EBMT); April 23-36, 2023; Paris, France.
- Risitano AM, Han B, Ueda Y, et al. Oral Complement Factor B Inhibitor Iptacopan Monotherapy Improves Hemoglobin to Normal/Near-Normal Levels in Paroxysmal Nocturnal Hemoglobinuria Patients Naïve to Complement Inhibitors: Phase III APPOINT-PNH Trial. Presented at: 49th Annual Meeting of the European Society for Blood and Marrow Transplantation (EBMT); April 23-36, 2023; Paris, France.
- Risitano AM, Röth A, Soret J, et al. Addition of iptacopan, an oral factor B inhibitor, to eculizumab in patients with paroxysmal nocturnal haemoglobinuria and active haemolysis: an open-label, single-arm, phase 2, proof-of-concept trial. Lancet Haematol. 2021;8(5):e344-e354. doi:10.1016/S2352-3026(21)00028-4
- Jang JH, Wong L, Ko BS, et al. Iptacopan monotherapy in patients with paroxysmal nocturnal hemoglobinuria: a 2-cohort open-label proof-of-concept study. Blood Adv. 2022;6(15):4450-4460. doi:10.1182/bloodadvances.2022006960
- Cançado RD, Araújo A da S, Sandes AF, et al. Consensus statement for diagnosis and treatment of paroxysmal nocturnal haemoglobinuria. Hematol Transfus Cell Ther. 2021;43(3):341-348. doi:10.1016/j.htct.2020.06.006
- McKinley CE, Richards SJ, Munir T, et al. Extravascular Hemolysis Due to C3-Loading in Patients with PNH Treated with Eculizumab: Defining the Clinical Syndrome. Blood. 2017;130(Supplement 1):3471. doi:10.1182/blood.V130.Suppl_1.3471.3471
- Dingli D, Matos JE, Lehrhaupt K, et al. The burden of illness in patients with paroxysmal nocturnal hemoglobinuria receiving treatment with the C5-inhibitors eculizumab or ravulizumab: results from a US patient survey. Ann Hematol. 2022;101(2):251-263. doi:10.1007/s00277-021-04715-5
- Novartis Pharmaceuticals. A Randomized, Multicenter, Active-Comparator Controlled, Open-Label Trial to Evaluate Efficacy and Safety of Oral, Twice Daily LNP023 in Adult Patients With PNH and Residual Anemia, Despite Treatment With an Intravenous Anti-C5 Antibody. clinicaltrials.gov; 2022. Accessed September 21, 2022. https://clinicaltrials.gov/ct2/show/NCT04558918
- Novartis Pharmaceuticals. A Multicenter, Single-Arm, Open-Label Trial to Evaluate Efficacy and Safety of Oral, Twice Daily Iptacopan in Adult PNH Patients Who Are Naive to Complement Inhibitor Therapy. clinicaltrials.gov; 2022. Accessed September 21, 2022. https://clinicaltrials.gov/ct2/show/NCT04820530
- Hill A, DeZern AE, Kinoshita T, Brodsky RA. Paroxysmal nocturnal haemoglobinuria. Nat Rev Dis Primer. 2017;3(1):17028. doi:10.1038/nrdp.2017.28
- Schrezenmeier H, Röth A, Araten DJ, et al. Baseline clinical characteristics and disease burden in patients with paroxysmal nocturnal hemoglobinuria (PNH): updated analysis from the International PNH Registry. Ann Hematol. 2020;99(7):1505-1514. doi:10.1007/s00277-020-04052-z
- Debureaux PE, Kulasekararaj AG, Cacace F, et al. Categorizing hematological response to eculizumab in paroxysmal nocturnal hemoglobinuria: a multicenter real-life study. Bone Marrow Transplant. 2021;56(10):2600-2602. doi:10.1038/s41409-021-01372-0
- Debureaux PE, Cacace F, Silva BGP, et al. Hematological Response to Eculizumab in Paroxysmal Nocturnal Hemoglobinuria: Application of a Novel Classification to Identify Unmet Clinical Needs and Future Clinical Goals. Blood. 2019;134(Supplement_1):3517-3517. doi:10.1182/blood-2019-125917
- Schubart A, Anderson K, Mainolfi N, et al. Small-molecule factor B inhibitor for the treatment of complement-mediated diseases. Proc Natl Acad Sci. 2019;116(16):7926-7931. doi:10.1073/pnas.1820892116
- Barratt J, Rovin B, Zhang H, et al. POS-546 EFFICACY AND SAFETY OF IPTACOPAN IN IgA NEPHROPATHY: RESULTS OF A RANDOMIZED DOUBLE-BLIND PLACEBO-CONTROLLED PHASE 2 STUDY AT 6 MONTHS. Kidney Int Rep. 2022;7(2):S236. doi:10.1016/j.ekir.2022.01.577
- Rizk DV, Rovin BH, Zhang H, et al. Targeting the Alternative Complement Pathway With Iptacopan to Treat IgA Nephropathy: Design and Rationale of the APPLAUSE-IgAN Study. Kidney Int Rep. 2023;8(5):968-979. doi:10.1016/j.ekir.2023.01.041
- Novartis investigational oral therapy iptacopan (LNP023) receives FDA Breakthrough Therapy Designation for PNH and Rare Pediatric Disease Designation for C3G. Novartis. Accessed September 22, 2022. https://www.novartis.com/news/media-releases/novartis-investigational-oral-therapy-iptacopan-lnp023-receives-fda-breakthrough-therapy-designation-pnh-and-rare-pediatric-disease-designation-c3g
- Novartis announces European Medicines Agency (EMA) has granted orphan drug designation for iptacopan (LNP023) in IgA nephropathy (IgAN). Novartis. Accessed September 22, 2022. https://www.novartis.com/news/media-releases/novartis-announces-european-medicines-agency-ema-has-granted-orphan-drug-designation-iptacopan-lnp023-iga-nephropathy-igan
- Novartis received European Medicines Agency (EMA) PRIME designation for iptacopan (LNP) in C3 glomerulopathy (C3G). Novartis. Accessed September 22, 2022. https://www.novartis.com/news/media-releases/novartis-received-european-medicines-agency-ema-prime-designation-iptacopan-lnp-c3-glomerulopathy-c3g
- Data on file. Novartis Pharmaceuticals Corp; 2023.
| Novartis Media Relations E-mail: [email protected]
|
|
| North America | |
| Julie Masow | +1 862 579 8456 |
| Michael Meo | +1 862 274 5414 |
| Marlena Abdinoor | +1 617 335 9525 |
Novartis Investor Relations E-mail: [email protected]
|
|
| North America | |
| Sloan Simpson | +1 862 345 4440 |
| Jonathan Graham | +1 201 602 9921 |
| Parag Mahanti | +1 973 876 4912 |
Resources for Media

Fabhalta® (iptacopan) packaging
Fabhalta® (iptacopan) packaging
Fabhalta® (iptacopan) fact sheet
Fabhalta® (iptacopan) fact sheet
Paroxysmal nocturnal hemoglobinuria (PNH) fact sheet
Paroxysmal nocturnal hemoglobinuria (PNH) fact sheet

Vinod Pullarkat, MD, MRCP, Clinical Professor, Department of Hematology and Hematopoietic Cell Transplantation, City of Hope
Vinod Pullarkat, MD, MRCP, Clinical Professor, Department of Hematology and Hematopoietic Cell Transplantation, City of Hope

Victor Bultó, President US, Novartis
Victor Bultó, President US, Novartis

Close up of the Novartis logo on the Banting 1 building, Novartis Campus Basel
Close up of the Novartis logo on the Banting 1 building, Novartis Campus Basel